 Figure 1A: Photograph of a lesion of the right lateral tongue with thickened leukoplakia and central depression.
Figure 1A: Photograph of a lesion of the right lateral tongue with thickened leukoplakia and central depression.
Mr. C, 46-year-old male with a history of aplastic anemia and allogeneic hematopoietic stem cell transplantation complicated by chronic graft versus host disease (GVHD) resulting in multiple past squamous cell carcinomas (SCC) of the oral cavity, presented with a new tongue lesion (Fig 1A).
Mr. C’s medical history included multiple resections of tongue and buccalmucosa cancers with reconstructions, a left neck dissection, and adjuvant radiotherapy. His course has been complicated by a difficult airway, vocal cord paralysis, an occluded left carotid stent, and a complex neck abscess requiring long-term antibiotic prophylaxis.
A new oral tongue lesion was first identified on a routine follow-up in January 2020. Mr. C was asymptomatic, without pain, bleeding or difficulty in eating. Exam demonstrated a lesion of the right lateral tongue with thickened leukoplakia and central depression. There was mild erythema of the mucosa but no erythroplakia. The left lateral tongue had minimal leukoplakia similar to prior exams. There were no palpable cervical lymph nodes or visible lesions on flexible nasopharyngolaryngoscopy.
On repeat exam a few weeks later, Mr. C reported new tongue tenderness, worse on the right side. The physical appearance of the lesion was unchanged other than mildly increased thickness. Given worsening symptoms, the decision was made to perform an in-office biopsy.
Biopsy of the tongue lesion revealed squamous cell carcinoma, at least in situ, and hyperkeratotic squamous mucosa with lichenoid chronic inflammation. Pathology noted that invasive cancer could not be excluded based on the biopsy specimen. We therefore planned a transoral partial glossectomy for excision of the new tongue lesion with intraoperative assessment of margins and possible split thickness skin graft.
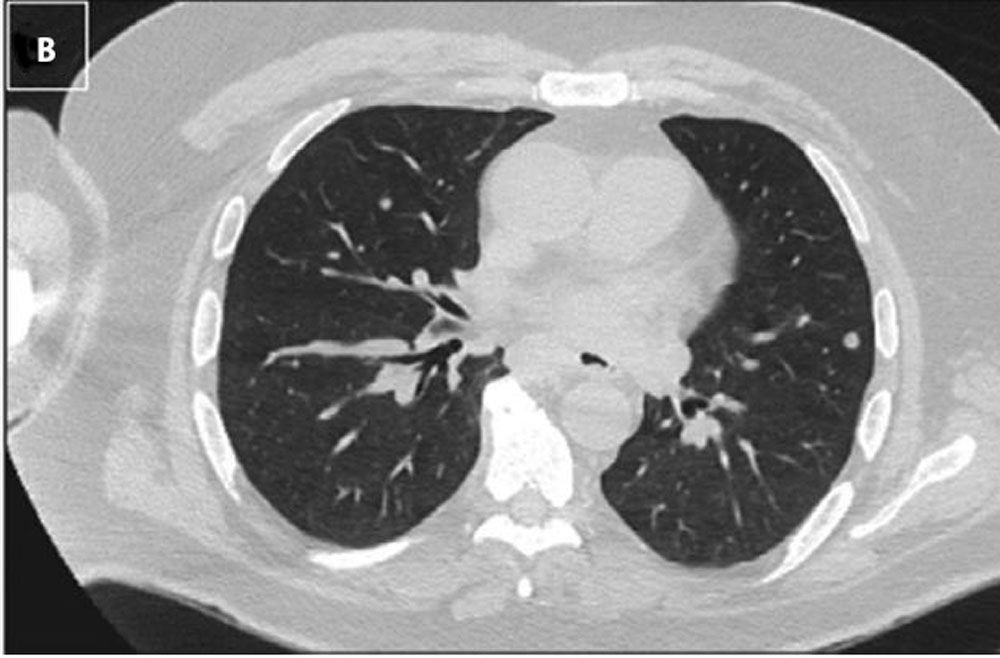 Figure 1B: Multiple new pulmonary nodules concerning for metastases.
Figure 1B: Multiple new pulmonary nodules concerning for metastases.
At this point, COVID-19 had entered our institution. Although surgery was the ideal approach to the diagnosis and treatment, we decided to delay intervention for the time being given his significant immunocompromised state and the small, relatively indolent nature of a lesion that could be monitored visually with relative ease. Mr. C is currently home quarantined with care coordinated via telemedicine including weekly photographic updates of the tongue lesion (Figure 1B).
This case appeared in a slightly different form in Head & Neck 2020;42:1131–1136.
Read other complex cases for head and neck cancer treatment during COVID
Management of Complex Head and Neck Cancers in the COVID Era – Case #1
Management of Complex Head and Neck Cancers in the COVID Era – Case #3